
What Determines Drug Dialyzability?

The extent of drug removal during dialysis determines whether supplemental dosing is necessary during or following dialysis. Dialysis of Drugs is provided as a general guide regarding the effect of dialysis on drug clearance.The drugs included in the table are parent drugs. A primary pharmacologically active or toxic metabolite is included in a few cases, but often little information is known. When available, serum drug measurements may be appropriate for dosing individual patients. In all cases, patients should be monitored for clinical efficacy and toxicity.The extent to which a drug is affected by dialysis is determined primarily by several physicochemical characteristics of the drug, including molecular size, protein binding, volume of distribution, water solubility, and plasma clearance. Technical aspects of the dialysis procedure and dialyzing membrane also may determine drug dialyzability.
Molecular Weight

The movement of drugs or other solutes is largely determined by the size of these molecules in relation to the pore size of the hemodialysis or peritoneal membrane. Generally, smaller molecular weight substances will pass through the membrane more easily than larger molecular weight substances. The pore size of the peritoneal membrane is generally considered to be larger than that of the hemodialysis membrane. Thus, larger molecular weight substances often cross the peritoneal membrane to a greater extent than the hemodialysis membrane.
Protein Binding
The concentration gradient of unbound (free) drug across the dialysis membrane affects drug dialyzability. Drugs with a high degree of protein binding will have a low plasma concentration of unbound drug available for dialysis. Uremia may have an effect on protein binding for some drugs, and, protein binding may decrease in uremic serum. Should this change in binding be substantial, increased dialyzability of free drug may occur.Because the primary binding proteins for most drugs (albumin, a1-acid glycoprotein) are of large molecular size, the drug-protein complex is often unable to cross the dialysis membrane, especially the hemodialysis membrane. Since the peritoneal membrane does permit the passage of some proteins, there may be some limited drug-protein removal with peritoneal dialysis. Increased protein concentrations often occur in peritoneal effluent during episodes of peritonitis.
Volume of Distribution
A drug with a large volume of distribution is dispersed widely throughout tissues and is present in relatively small amounts in the blood. Factors that contribute to a large volume of distribution include a high degree of lipid solubility and low plasma protein binding. Drugs with a large volume of distribution are likely to be dialyzed minimally.
Water Solubility
Dialysis fluids are aqueous solutions. Thus, in general, drugs with high water solubility will be dialyzed to a greater extent than those with high lipid solubility. Highly lipid-soluble drugs tend to be distributed throughout tissues, and therefore only a small fraction of the drug is present in plasma and accessible for dialysis.
Plasma Clearance
The inherent metabolic clearance—the sum of renal and nonrenal clearance—is often termed the “plasma clearance” of a drug. In dialysis patients, renal clearance is largely replaced by dialysis clearance. If nonrenal clearance is large compared to renal clearance, the contribution of dialysis to total drug removal is low. However, if renal (dialysis) clearance increases plasma clearance by 30% or more, dialysis clearance is considered to be clinically important.
Dialysis Membrane

Pore size, surface area, and geometry are the primary determinants of the performance of dialysis membranes. The technology of dialysis membranes is continuously evolving. Contemporary hemodialysis membranes may have very different drug dialysis characteristics than those used in previous decades. Thus, interpretation of older published literature should be tempered accordingly.
Blood and Dialysate Flow Rates
An individual hemodialysis prescription includes blood and dialysate flow rates. In general, increased blood flow rates will deliver greater amounts of drug to the dialysis membrane. As the drug concentration increases in the dialysate, the flow rate of the dialysis solution also becomes important in overall drug removal. Greater dialysis can be achieved with faster dialysate flow rates that keep the dialysate drug concentration at a minimum.Peritoneal blood flow rates generally are unable to be altered during peritoneal dialysis. However, dialysate flow rates are determined by the volume and frequency of dialysate exchanges in the peritoneum. At low exchange rates, drug concentrations in the dialysate will increase during the time in which the dialysate resides in the peritoneum, thus slowing additional movement of drug across the membrane. More frequent exchanges will generally favor increased drug dialyzability.
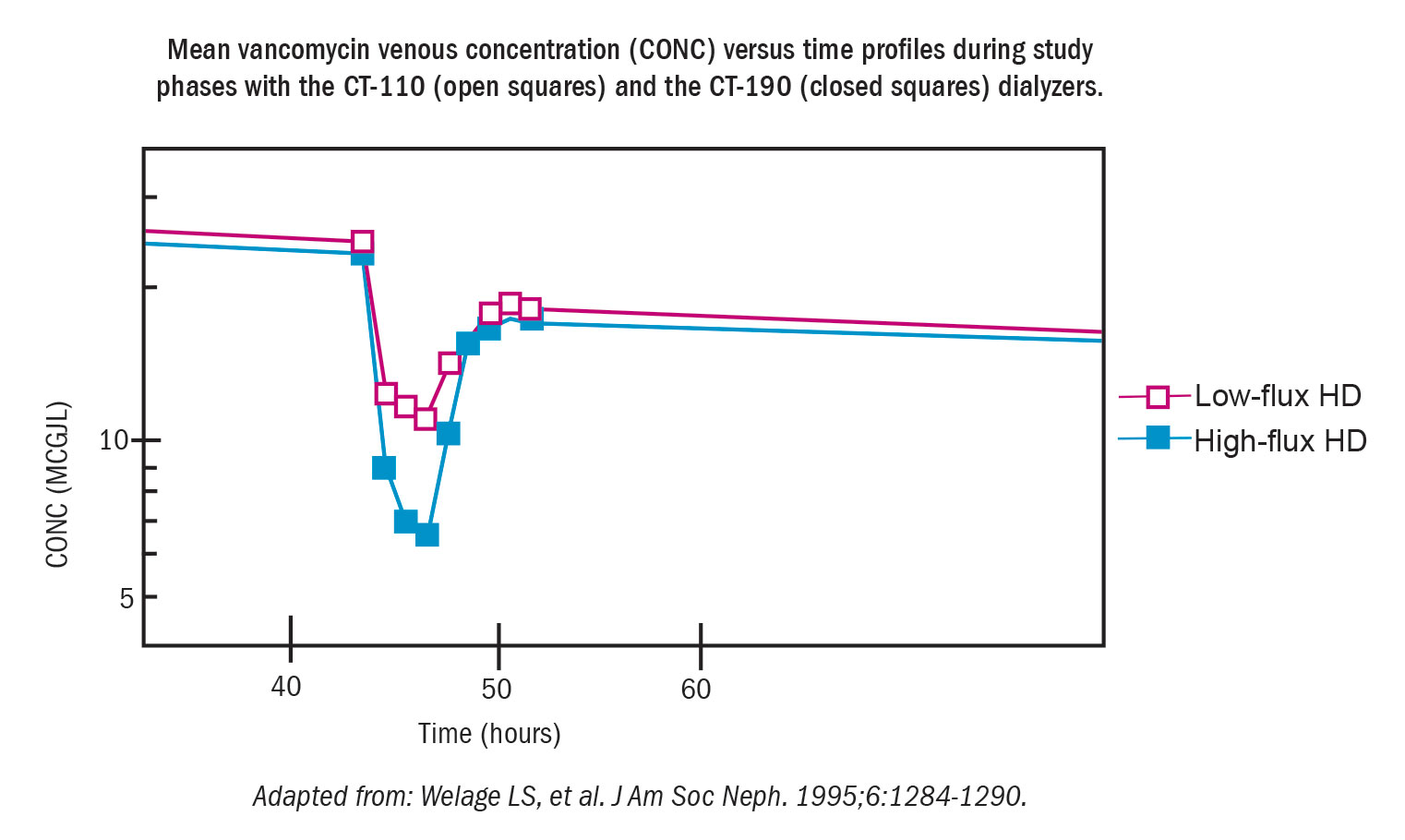
High Permeability Dialysis
Much of the information contained in this guide has been obtained from early studies (1970s to 1990s) conducted under conditions of standard hemodialysis using conventional dialysis membranes. Contemporary hemodialysis uses more permeable dialysis membranes and higher blood and dialysate flow rates, often referred to as “high permeability,” “high-efficiency,” and “high-flux” dialysis. The United States Food and Drug Administration has classified high permeability dialysis membranes as those whose in vitro ultrafiltration coefficient (KUf) is greater than 8 mL/hour/mm Hg. Changes in dialysis membranes and changes in blood and dialysis flow rates may have clinically important effects on drug removal through the membrane, and drug removal from plasma is often enhanced compared with more conventional dialysis membranes. High permeability dialysis may remove drug from plasma at a rate exceeding the transfer of drug from tissues to plasma. As a result, a rebound of plasma drug concentrations following the conclusion of dialysis may occur as blood-tissue drug equilibration occurs. Patients receiving high permeability dialysis may require more drug compared with those receiving standard hemodialysis. Therefore, individualized therapeutic drug monitoring may be necessary. The reader is referred to the primary literature for further details.No information is provided on drug dialyzability with continuous renal replacement therapy or with plasmapheresis due to multiple different techniques and a lack of standardization in practice.
Summary

Drug dialyzability is determined by a complex interaction of many factors, including the characteristics of the drug and the technical aspects of the dialysis system. Published studies on drug dialyzability should specify the conditions that pertain during dialysis. Results from these studies should be applied with caution to other dialysis conditions.